
Prostate cancer is the most common type of cancer in men in the United States (other than skin cancer). On average, one man in nine will be diagnosed with prostate cancer during his lifetime; however, only 17% of men diagnosed with prostate cancer will die from it.
Prostate cancer is more likely to be diagnosed in older men and African-American men. The risk of prostate cancer increases with age, and it affects 6 out of every 10 men over the age of 65. The average age at diagnosis is 66 and the disease is very rare in men under the age of 40.
The prostate is a gland in the male reproductive system that secretes prostate fluid, a milky white, alkaline substance that nourishes and protects sperm and makes up about one-third of the volume of semen.
The prostate gland is normally about the size of a walnut and surrounds the upper part of the urethra, the tube that empties urine from the bladder and which sperm travels down during ejaculation. If the prostate gland grows too large it can affect the flow of both urine and sperm.

What is Prostate Cancer?
Billions of cells make up the human body and sometimes these cells reproduce in an uncontrolled way, forming a lump of tissue that may be described as a tumor.
There are two types of tumor, benign and malignant.
Benign tumors do not spread to other parts of the body and they are rarely life-threatening. Benign prostatic hyperplasia (BPH) is a condition characterized by the abnormal growth of prostate cells. In BPH, the prostate grows larger and presses against the urethra and bladder, interfering with the normal flow of urine. It is not usually life-threatening; however, it can significantly affect a man’s quality of life and lead to other serious problems such as incontinence, urinary retention (when you are unable to empty your bladder), urinary tract infections, and rarely bladder or kidney damage.
Malignant tumors are cancer. The cells in these tumors divide without control or order and can attack nearby normal cells and destroy them. Cells can also break away from the tumor and spread to other parts of the body via the blood or lymphatic system, forming satellite tumors, called secondary cancers or metastases. If somebody is found to have secondary tumors in other areas of their body such the lymph nodes, bone, bladder, or rectum, they are said to have metastatic prostate cancer.
Most men who develop prostate cancer are over the age of 65 and 90% of prostate cancers are found when the cancer is only in the prostate or nearby organs (this is called localized prostate cancer). Almost 100% of men diagnosed with localized prostate cancer are still alive 5 years after the diagnosis. For those men diagnosed with prostate cancer that has spread to other parts of the body, the 5-year survival rate is 31%.
Very old men who develop prostate cancer are more likely to have very slow growing tumors with few or no symptoms.
What causes Prostate Cancer?
Although doctors do not know what causes prostate cancer, they do know that testosterone stimulates prostate cancer growth. Other risk factors include:
- Age -- In the United States, about six in 10 cases of prostate cancer are found in men older than 65. Prostate cancer is rare in men younger than 40
- A family history of prostate cancer – Having a father or brother who has had prostate cancer more than doubles the risk of developing the disease. If several relatives have been affected, the risk is even higher, particularly if they developed it young
- Race -- Prostate cancer is much more common in African-American men and Caribbean men of African origin. African-American men are more than twice as likely to die from prostate cancer as white men. Prostate cancer is less common in Asian-American, Hispanic-Latino and Native American men than in white men
- Geography – Prostate Cancer is more common in North America, Australia, the Caribbean Islands and North-western Europe and less common in Asia, Africa, Central America and South America. Asian-American men are more likely to develop prostate cancer than Asian men of similar backgrounds living in Asia.
There is some evidence that inherited gene mutations (such as the BRCA2 gene) may increase the risk of prostate cancer in some men. In addition, some conditions, such as hereditary non-polyposis colorectal cancer (Lynch syndrome) carry an increased risk of several cancers, including prostate cancer.
Other factors which may or may not have an effect on prostate cancer risk include:
- Diet: The risk of prostate cancer is slightly higher in men who eat a lot of red meat or high-fat dairy products; however, these men also tend to eat fewer fruits and vegetables, and doctors are not sure which factor is responsible for increasing the risk
- Obesity: Some studies have reported that obese men are more likely to develop aggressive prostate cancer, die from the condition, or be diagnosed at a more advanced stage; however, they are less likely to develop a low-grade (less dangerous) form of the disease
- Chemical exposure: Firefighters and Vietnam War vets exposed to Agent Orange appear to have an increased risk of prostate cancer, although not all studies have reported an increased risk.
No conclusive increase in risk has been reported with smoking, inflammation of the prostate, sexually transmitted infections, or in men who have had a vasectomy.
Can Prostate Cancer Be Found Early?
Screening for prostate cancer is a little bit controversial because experts are unsure whether the benefits of testing all men for prostate cancer outweigh the risks, such as finding and treating cancers that probably would have never caused any problems. Your doctor will advise you of the risks and potential benefits for you of screening for prostate cancer.
There are two tests that may be used either for screening or for investigating symptoms suggestive of prostate cancer.
- A blood test for Prostate Specific Antigen (PSA). PSA is a protein produced by normal as well as malignant cells of the prostate gland. A PSA test measures the level of this protein in the blood. Men with prostate cancer often have elevated PSA levels in their blood; however, levels may also become elevated for a number of other reasons, such as prostatitis (inflammation of the prostate) and benign prostatic hyperplasia (BPH), so an elevated PSA does not mean a man has prostate cancer. In addition, PSA levels may be lowered in men prescribed medicines such as finasteride, dutasteride, aspirin, statins, or thiazide diuretics; taking herbal supplements; or who are obese.
- A digital rectal exam (DRE) involves the doctor inserting a lubricated, gloved finger into the rectum to feel the prostate through the rectal wall and to check for hard or lumpy areas. A DRE may be used to screen for or used to help diagnose prostate problems.
Symptoms of Prostate Cancer
Some prostate cancers are so small that they cannot be felt during a routine rectal examination and may not cause any symptoms. Symptoms usually start when the prostate cancer grows so much that it starts to squeeze the urethra, which it surrounds. Symptoms may include:
- A need to urinate frequently, especially at night
- A painful or burning feeling when urinating
- An inability to urinate
- Blood in the urine or semen
- Difficulty in obtaining an erection
- Difficulty in starting urination or holding back urine
- Frequent pain or stiffness in the lower back, hips, or upper thighs
- Painful ejaculation
- A weak or spasmodic flow of urine.
Many of these symptoms are common to other prostate problems, not just prostate cancer. If you experience any of these symptoms you should see your doctor or urologist.
Diagnosing Prostate Cancer

If your symptoms or initial test results suggest prostate cancer, then your doctor will conduct other tests, such as a transrectal ultrasound (TRUS) and a prostate biopsy.
During a TRUS, a small probe about the width of a finger is placed in the rectum that uses ultrasound waves to create a black and white picture of your prostate. The procedure usually takes around 10 minutes.
A prostate biopsy involves inserting a thin hollow needle through the wall of the rectum and into the prostate to take a small sample of prostate tissue. The tissue can then be examined for cancer cells in a laboratory. A local anesthetic is usually used to numb the area first, and the procedure is usually done during a TRUS.
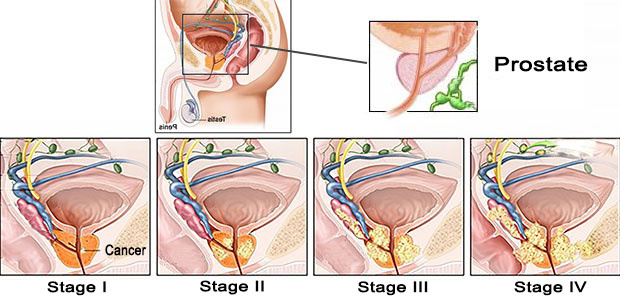
Stages of Prostate Cancer
If cancer is found in the prostate, the doctor needs to know the stage or extent of the disease.
The most widely used staging system is the AJCC (American Joint Committee on Cancer) TNM staging system. This is based on five key pieces of information:
- T: The extent of the primary tumor
- N: If the cancer has spread to nearby lymph nodes
- M: If the cancer has metastasized
- The PSA level at the time of diagnosis
- The Grade Group, which is a measure of how likely the cancer is to grow and spread quickly and is determined by the results of a prostate biopsy or surgery (calculated as the Gleason score).
Prostate cancer staging can be complex, and you should ask your doctor or somebody on your cancer care team to explain it to you in an easy to understand way.
Methods of Treatment and Side Effects
Not every man with prostate cancer requires treatment.
Doctors will take into consideration your age and your general health as well as the stage of your cancer and how likely it is to cause problems for you. Most treatments have some side effects, so it is important that you ask as many questions as you need to and talk with your family and friends before making any decisions about treatment.
A lot of your decision depends upon your desires as an individual, for example, if you want the cancer out of your body immediately, no matter the consequences. There are also other factors to consider, such as do you go with new technology such as robotic surgery or proton beam radiation therapy, or more traditional treatment that has well-proven results. The decision is often not an easy one, and you should take some time to make the right decision for you based on your doctor’s recommendations.
The following are common treatment options that may be offered:
- Watchful waiting: For older men with other serious health issues and low-grade prostate cancer this may be the preferred option. Your doctor will still monitor your cancer for growth or other changes, but no treatment is prescribed. If symptoms become troublesome, your doctor may recommend you start treatment
- Surgery: A common option for early-stage prostate cancer, during which some or all the prostate is removed, depending on the procedure. Post-surgical pain is common and there is a risk of long-term problems such as erectile dysfunction, rectal injury, and urinary incontinence
- Radiation therapy (called radiotherapy): External radiation uses a high-energy x-ray which is directed at the area of the prostate affected by cancer. Internal or implant radiation (also called brachytherapy) uses tiny radioactive implants that are placed inside or near the tumor. Usually only used to treat small tumors or in advanced disease for pain relief. Side effects include extreme fatigue, diarrhea, erectile dysfunction, and frequent or uncomfortable urination
- Hormonal therapy: Uses medicines to prevent the production of testosterone or block the action of testosterone which deprives the cancer cells of the male hormones they need to grow. Surgery to remove the testes (orchidectomy) is also a way of depriving the cancer of testosterone. Usually used to treat prostate cancer that has spread, or to prevent its return following surgery or radiation treatment
- Chemotherapy: Not usually a standard treatment for early prostate cancer, but some studies are investigating its effect when given for a short time after surgery
- Vaccine treatment: Sipuleucel-T (Provenge) boosts the immune system to help it attack prostate cancer cells. Each vaccine is made specifically for each man and is used to treat advanced prostate cancer that is no longer responding to hormone therapy
- Bone-directed treatment: If prostate cancer spreads it nearly always goes to the bones first. Treatments may include analgesics, hormone therapy, chemotherapy, vaccines, bisphosphonates (eg, zoledronic acid [Reclast, Zometa]), denosumab (Xgeva, Prolia), and radiation therapy.
Drugs used in the Treatment of Prostate Cancer
Luteinizing hormone-releasing hormone (LHRH) agonists
These lower the amount of testosterone made by the testicles.
|
Generic name |
Brand name examples |
|---|---|
|
goserelin implant |
Zoladex |
|
histrelin implant |
Vantus |
|
leuprolide injection |
Eligard, Lupron Depot |
|
triptorelin |
Trelstar |
Luteinizing hormone-releasing hormone (LHRH) antagonists
These lower testosterone levels more quickly than LHRH agonists but without causing a tumor flare. Usually only used to treat advanced prostate cancer.
|
Generic name |
Brand name examples |
|---|---|
|
degarelix |
Firmagon |
CYP17 inhibitors
These block an enzyme called CYP17 that makes androgens in prostate cells. Usually reserved for high-risk or castrate-resistant prostate cancer. Usually used in combination with other treatments.
|
Generic name |
Brand name examples |
|---|---|
|
abiraterone |
Zytiga |
Antiandrogens
These block the action of androgens (male hormones), including testosterone.
|
Generic name |
Brand name examples |
|---|---|
|
bicalutamide |
Casodex |
|
flutamide |
Eulexin |
|
nilutamide |
Nilandron |
Newer antiandrogens that have a similar effect but work by a different mechanism and may be used for castration-resistant prostate cancer (CRPC) or metastatic castration-sensitive prostate cancer (mCSPC) include:
- enzalutamide (Xtandi)
- apalutamide (Erleada).
Other medicines with an antiandrogen effect
The following medicines may also be considered for the treatment of prostate cancer.
|
Generic name |
Comments |
|---|---|
|
aminoglutethimide |
Prevents androgen production by the adrenal cortex |
|
estrogens |
May be considered when other treatments have failed. Side effects include blood clots and breast enlargement |
|
ketoconazole (Nizoral) |
An antifungal agent that also blocks the production of androgens. Not FDA approved for use in prostate cancer |
Chemotherapy agents
Trials are investigating the effectiveness of chemotherapy agents for prostate cancer. They are typically used one at a time.
|
Generic name |
Brand name examples |
|---|---|
|
cabazitaxel |
Jevtana |
|
docetaxel |
Taxotere |
|
estramustine |
Emcyt |
|
mitoxantrone |
Novantrone |
What can I do to manage my prostate cancer?
- Do not smoke. Nicotine can damage blood vessels and make it more difficult to manage your prostate cancer. Smoking also increases your risk for new or returning cancer and delays healing after treatment. Do not use e-cigarettes or smokeless tobacco in place of cigarettes or to help you quit. They still contain nicotine. Ask your healthcare provider for information if you currently smoke and need help quitting.
- Limit or do not drink alcohol as directed. A drink is 12 ounces of beer, 1½ ounces of liquor, or 5 ounces of wine.
- Eat a variety of healthy foods. Healthy foods include fruits, vegetables, whole-grain breads, low-fat dairy products, beans, lean meats, and fish. Your healthcare provider may also recommend changes to the amounts of calcium and vitamin D you have each day.
- Manage your weight. Obesity may increase your risk for problems from prostate cancer. Limit or do not have high-calorie foods or drinks.
- Exercise as directed. Exercise may help you recover after treatment and may help prevent your prostate cancer from returning. Exercise can also help you manage your weight. Try to get at least 30 minutes of exercise 5 days a week, such as walking.
- Ask about sexual activity. Ask your healthcare provider when it is safe for you to start having sex after your treatment. Medicines may be given if you have trouble getting or maintaining an erection.
- Manage incontinence. You may have incontinence (trouble controlling when you urinate) after treatment. Ask your healthcare provider for information on managing urinary incontinence. You may be able to gain control over your urination with techniques or medicines.
- Drink liquids as directed. Ask how much liquid to drink each day and which liquids are best for you. Drink extra liquids to prevent dehydration. You will also need to replace fluid if you are vomiting or have diarrhea from cancer treatments.