Generic name: levonorgestrel / ethinyl estradiol and ethinyl estradiol
Dosage form: tablets
Drug class: Contraceptives
Note: This document contains side effect information about ethinyl estradiol / levonorgestrel. Some of the dosage forms listed on this page may not apply to the brand name Jaimiess.
WARNING: CIGARETTE SMOKING AND SERIOUS CARDIOVASCULAR EVENTS
Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptives (COC) use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, COCs should not be used by women who are over 35 years of age and smoke. [See CONTRAINDICATIONS
For the Consumer
Applies to ethinyl estradiol / levonorgestrel: oral tablet
Warning
Oral route (Tablet)
Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptives (COC) use. This risk increases with age, particularly in women older than 35 years, and with the number of cigarettes smoked. Women who use oral contraceptives should be strongly advised not to smoke.
Side effects requiring immediate medical attention
Along with its needed effects, ethinyl estradiol/levonorgestrel may cause some unwanted effects. Although not all of these side effects may occur, if they do occur they may need medical attention.
Check with your doctor immediately if any of the following side effects occur while taking ethinyl estradiol / levonorgestrel:
Incidence not known
- Absent, missed, or irregular menstrual periods
- anxiety
- bloody stools
- blurred vision
- breast tenderness, enlargement, discharge
- changes in skin color, pain, tenderness, or swelling of the foot or leg
- chest pain or discomfort
- chills
- clay-colored stools
- confusion
- cough
- dark or cloudy urine
- decrease in urine output or decrease in urine-concentrating ability
- diarrhea
- difficult, burning, or painful urination
- difficulty in speaking
- dizziness or lightheadedness
- double vision
- dull ache or feeling of pressure or heaviness in the legs
- fainting
- fast heartbeat
- fever
- fluid-filled skin blisters
- frequent urge to urinate
- headache, severe and throbbing
- inability to move the arms, legs, or facial muscles
- inability to speak
- itching of the vagina or outside the genitals
- itching skin near damaged veins
- light vaginal bleeding between regular menstrual periods
- loss of appetite
- nausea
- nervousness
- pain during sexual intercourse
- pain or discomfort in the arms, jaw, back or neck
- pelvic pain
- pounding in the ears
- sensitivity to the sun
- skin thinness
- slow or fast heartbeat
- slow speech
- stomach bloating and cramping
- stomach pain and tenderness
- stopping of menstrual bleeding
- sweating
- swelling, pain, or tenderness in the upper abdominal area
- swollen feet and ankles
- tenderness, pain, swelling, warmth, skin discoloration, and prominent superficial veins over the affected area
- thick, white curd-like vaginal discharge without odor or with mild odor
- troubled breathing
- twitching, uncontrolled movements of the tongue, lips, face, arms, or legs
- unpleasant breath odor
- unusual tiredness or weakness
- vomiting
- vomiting of blood
- yellow eyes or skin
Side effects not requiring immediate medical attention
Some side effects of ethinyl estradiol / levonorgestrel may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects.
Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them:
Incidence not known
- Acne
- changes in appetite
- changes in weight
- decreased interest in sexual intercourse
- decreased milk production
- loss in sexual ability, desire, drive, or performance
- mental depression
- patchy brown or dark brown discoloration of the skin
Managing side effects (general information)
For Healthcare Professionals
Applies to ethinyl estradiol / levonorgestrel: oral tablet, transdermal film
General
The most frequently reported side effects were headache, heavy/irregular vaginal bleeding, nausea/vomiting, acne, dysmenorrhea, weight increased, mood changed, anxiety/panic attack, breast pain, and migraines.[Ref]
Genitourinary
Very common (10% or more): Irregular/heavy uterine bleeding (up to 17%), menorrhagia (up to 11.6%), breast pain (up to 11.2%), dysmenorrhea (up to 11%), breakthrough bleeding/spotting
Common (1% to 10%): Breast tenderness/discomfort, vaginitis, candidiasis, breast enlargement, breast secretion, breast tension, intermenstrual bleeding/metrorrhagia
Uncommon (0.1% to 1%): Breast enlargement, breast hypertrophy, menstrual flow changed
Rare (less than 0.1%): Breast discharge, vaginal discharge, amenorrhea
Frequency not reported: Uterine myoma, temporary infertility, cervical erosion changed, cervical secretion changed, diminution in lactation
Postmarketing reports: Menstrual flow reduced, withdrawal bleeding missed, post pill amenorrhea
Cardiovascular
Uncommon (0.1% to 1%): Blood pressure increased
Rare (less than 0.1%): Venous thromboembolism, arterial thromboembolism
Frequency not reported: Deep vein thrombosis, hypertension, myocardial infarction, varicose veins exacerbated, thrombophlebitis, cerebral vascular disease, mitral valve prolapse
Postmarketing reports: Thrombosis
Nervous system
Very common (10% or more): Headache (up to 33%)
Common (1% to 10%): Migraine, dizziness
Very rare (less than 0.01%): Chorea exacerbated
Frequency not reported: Loss of consciousness, epilepsy, Sydenham's chorea, transient ischemic attack, ischemic stroke, hemorrhagic stroke, stroke, cerebral hemorrhage, cerebral thrombosis
Gastrointestinal
Very common (10% or more): Nausea/vomiting (up to 11%)
Common (1% to 10%): Abdominal pain/cramps, diarrhea
Very rare (less than 0.01%): Pancreatitis
Frequency not reported: Crohn's disease, ulcerative colitis, bloating, mesenteric thrombosis
Postmarketing reports: Abdominal distention
Oncologic
Rare (less than 0.1%): Benign liver tumor, malignant liver tumor, breast cancer
Hepatic
Rare (less than 0.1%): Cholestatic jaundice
Very rare (less than 0.01%): Gallbladder disease, gallbladder disease exacerbated
Frequency not reported: Cholecystitis, cholelithiasis, Budd-Chiari syndrome
Postmarketing reports: Liver function disturbance
Hematologic
Frequency not reported: Hemolytic uremic syndrome
Psychiatric
Common (1% to 10%): Mood changed, mood swings/alteration/affect lability, depression, anxiety/panic attack, nervousness, libido decreased, libido increased, depression
Frequency not reported: Major depressive disorder, suicide attempt, depressed mood, crying, major depression, affective disorder, depression suicidal, dysthymic disorder
Postmarketing reports: Insomnia
Immunologic
Rare (less than 0.1%): Hypersensitivity reaction, anaphylactic/anaphylactoid reaction
Very rare (less than 0.01%): Systemic lupus erythematosus exacerbated
Ocular
Rare (less than 0.1%): Contact lens intolerance
Very rare (less than 0.01%): Retinal vein thrombosis
Frequency not reported: Cataract, corneal curvature changed/steepening
Postmarketing reports: Optic neuritis
Metabolic
Common (1% to 10%): Appetite increased, fluid retention/edema
Uncommon (0.1% to 1%): Appetite decreased, serum lipid levels changed, hypertriglyceridemia
Rare (less than 0.1%): Glucose tolerance changed
Frequency not reported: Tolerance to carbohydrates reduced
Dermatologic
Common (1% to 10%): Acne
Uncommon (0.1% to 1%): Urticaria, rash, chloasma
Rare (less than 0.1%): Erythema nodosum, erythema multiforme, hereditary angioedema exacerbated
Frequency not reported: Herpes gestationis, hirsutism, alopecia, melasma
Postmarketing reports: Alopecia, itching, angioedema[Ref]
Other
Common (1% to 10%): Weight gain, weight changed, flu syndrome
Rare (less than 0.1%): Weight decreased
Very rare (less than 0.01%): Porphyria exacerbated
Frequency not reported: Ectopic pregnancy, spontaneous abortion, porphyria, congenital anomaly, cystitis-like syndrome
Postmarketing reports: Chest pain, fatigue, malaise, edema peripheral, pain, serum folate decreased
Musculoskeletal
Common (1% to 10%): Back pain
Frequency not reported: Systemic lupus erythematosus
Postmarketing reports: Muscle spasm, pain in extremity
Renal
Frequency not reported: Pulmonary embolism
Postmarketing reports: Pulmonary thrombosis
Indications and Usage for Jaimiess
Jaimiess is indicated for use by women to prevent pregnancy.
Jaimiess Dosage and Administration
Take one tablet by mouth at the same time every day. The dosage of Jaimiess are one peach tablet containing levonorgestrel and ethinyl estradiol daily for 84 consecutive days, followed by one yellow ethinyl estradiol tablet for 7 days. To achieve maximum contraceptive effectiveness, Jaimiess must be taken exactly as directed and at intervals not exceeding 24 hours.
Instruct the patient to begin taking Jaimiess on the first Sunday after the onset of menstruation. If menstruation begins on a Sunday, the first peach tablet is taken that day. One peach tablet should be taken daily for 84 consecutive days, followed by one yellow tablet for 7 consecutive days. A non-hormonal back-up method of contraception (such as condoms or spermicide) should be used until a peach tablet has been taken daily for 7 consecutive days. A scheduled period should occur during the 7 days that the yellow tablets are taken.
Begin the next and all subsequent 91-day cycles without interruption on the same day of the week (Sunday) on which the patient began her first dose of Jaimiess following the same schedule: 84 days taking a peach tablet followed by 7 days taking a yellow tablet. If the patient does not immediately start her next pill pack, she should protect herself from pregnancy by using a non-hormonal back-up method of contraception until she has taken a light blue-green tablet daily for 7 consecutive days.
If unscheduled spotting or bleeding occurs, instruct the patient to continue on the same regimen. If the bleeding is persistent or prolonged, advise the patient to consult her healthcare provider.
For postpartum women who are not breastfeeding, start Jaimiess no earlier than four to six weeks postpartum due to increased risk of thromboembolism. If the patient starts on Jaimiess postpartum and has not yet had a period, evaluate for possible pregnancy, and instruct her to use an additional method of contraception until she has taken a peach tablet for 7 consecutive days.
Dosage Forms and Strengths
Jaimiess tablets (levonorgestrel/ethinyl estradiol tablets, USP and ethinyl estradiol tablets, USP) are available in extended-cycle blister cards, each containing a 13-week supply of tablets: 84 peach tablets, each containing 0.15 mg of levonorgestrel and 0.03 mg ethinyl estradiol, and 7 yellow tablets each containing 0.01 mg of ethinyl estradiol. The peach tablets are round, film-coated, debossed with SZ on one side and J4 on the other side. The yellow tablets are round, film-coated, debossed with SZ on one side and L1 on the other side.
Warnings and Precautions
Thrombotic and Other Vascular Events
Stop Jaimiess if an arterial or deep venous thrombotic event occurs. Although the use of COCs increases the risk of venous thromboembolism, pregnancy increases the risk of venous thromboembolism as much or more than the use of COCs. The risk of venous thromboembolism in women using COCs is 3 to 9 per 10,000 woman-years. The excess risk is highest during the first year of use of a COC. Use of COCs also increases the risk of arterial thromboses such as strokes and myocardial infarctions, especially in women with other risk factors for these events. The risk of thromboembolic disease due to COCs gradually disappears after COC use is discontinued.
Use of Jaimiess provides women with more hormonal exposure on a yearly basis than conventional monthly oral contraceptives containing the same strength synthetic estrogens and progestins (an additional 9 and 13 weeks of exposure to progestin and estrogen, respectively, per year).
If feasible, stop Jaimiess at least 4 weeks before and through 2 weeks after major surgery or other surgeries known to have an elevated risk of thromboembolism.
Start Jaimiess no earlier than 4 to 6 weeks after delivery, in women who are not breastfeeding. The risk of postpartum thromboembolism decreases after the third postpartum week, whereas the risk of ovulation increases after the third postpartum week.
COCs have been shown to increase both the relative and attributable risks of cerebrovascular events (thrombotic and hemorrhagic strokes), although, in general, the risk is greatest among older (>35 years of age), and hypertensive women who also smoke. COCs also increase the risk for stroke in women with other underlying risk factors.
Oral contraceptives must be used with caution in women with cardiovascular disease risk factors.
Stop Jaimiess if there is unexplained loss of vision, proptosis, diplopia, papilledema, or retinal vascular lesions. Evaluate for retinal vein thrombosis immediately.
Carcinoma of the Breast and Cervix
Women who currently have or have had breast cancer should not use Jaimiess because breast cancer may be hormonally sensitive.
There is substantial evidence that COCs do not increase the incidence of breast cancer. Although some past studies have suggested that COCs might increase the incidence of breast cancer, more recent studies have not confirmed such findings.
Some studies suggest that COCs are associated with an increase in the risk of cervical cancer or intraepithelial neoplasia. However, there is controversy about the extent to which these findings are due to differences in sexual behavior and other factors.
Liver Disease
Discontinue Jaimiess if jaundice develops. Steroid hormones may be poorly metabolized in patients with impaired liver function. Acute or chronic disturbances of liver function may necessitate the discontinuation of COC use until markers of liver function return to normal and COC causation has been excluded.
Hepatic adenomas are associated with COC use. An estimate of the attributable risk is 3.3 cases/100,000 COC users. Rupture of hepatic adenomas may cause death through intra-abdominal hemorrhage.
Studies have shown an increased risk of developing hepatocellular carcinoma in long-term (> 8 years) COC users. However, the attributable risk of liver cancers in COC users is less than one case per million users.
Oral contraceptive-related cholestasis may occur in women with a history of pregnancy-related cholestasis. Women with a history of COC-related cholestasis may have the condition recur with subsequent COC use.
Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment
During clinical trials with the Hepatitis C combination drug regimen that containsobmitasvir/paritaprevir/ritonavir, with or without dasabuvir, ALT elevations greater than 5 times theupper limit of normal (ULN), including some cases greater than 20 times the ULN, weresignificantly more frequent in women using ethinyl estradiol-containing medications, such as COCs. Discontinue Jaimiess prior to starting therapy with the combination drug regimenombitasvir/paritaprevir/ritonavir, with or without dasabuvir
Jaimiess can be restarted approximately 2 weeks following completion of treatment with theHepatitis C combination drug regimen.
High Blood Pressure
For women with well-controlled hypertension, monitor blood pressure and stop Jaimiess if blood pressure rises significantly. Women with uncontrolled hypertension or hypertension with vascular disease should not use COCs.
An increase in blood pressure has been reported in women taking COCs, and this increase is more likely in older women and with extended duration of use. The incidence of hypertension increases with increasing concentration of progestin.
Gallbladder Disease
Studies suggest a small increased relative risk of developing gallbladder disease among COC users.
Carbohydrate and Lipid Metabolic Effects
Carefully monitor prediabetic and diabetic women who are taking Jaimiess. COCs may decrease glucose tolerance in a dose-related fashion.
Consider alternative contraception for women with uncontrolled dyslipidemias. A small proportion of women will have adverse lipid changes while on COCs.
Women with hypertriglyceridemia, or a family history thereof, may be at an increased risk of pancreatitis when using COCs.
Headache
If a woman taking Jaimiess develops new headaches that are recurrent, persistent, or severe, evaluate the cause and discontinue Jaimiess if indicated.
An increase in frequency or severity of migraine during COC use (which may be prodromal of a cerebrovascular event) may be a reason for immediate discontinuation of the COC.
Bleeding Irregularities
Unscheduled (breakthrough) bleeding and spotting sometimes occur in patients on COCs, especially during the first 3 months of use. If bleeding persists, check for causes such as pregnancy or malignancy. If pathology and pregnancy are excluded, bleeding irregularities may resolve over time or with a change to a different COC.
When prescribing Jaimiess, the convenience of fewer planned menses (4 per year instead of 13 per year) should be weighed against the inconvenience of increased unscheduled bleeding and/or spotting. The primary clinical trial (PSE-301) that evaluated the efficacy of levonorgestrel/ethinyl estradiol and ethinyl estradiol also assessed unscheduled bleeding. The participants in the 12-month clinical trial (N=1,006) completed the equivalent of 8,681 28-day cycles of exposure and were composed primarily of women who had used oral contraceptives previously (89%) as opposed to new users (11%). A total of 82 (8.2%) of the women discontinued levonorgestrel/ethinyl estradiol and ethinyl estradiol, at least in part, due to bleeding or spotting.
Scheduled (withdrawal) bleeding and/or spotting remained fairly constant over time, with an average of 3 days of bleeding and/or spotting per each 91-day cycle. Unscheduled bleeding and unscheduled spotting decreased over successive 91-day cycles. Table 1 below presents the number of days with unscheduled bleeding in treatment cycles 1 and 4. Table 2 presents the number of days with unscheduled spotting in treatment cycles 1 and 4.
| Q1=Quartile 1: 25% of women had ≤ this number of days of unscheduled bleeding Median: 50% of women had ≤ this number of days of unscheduled bleeding Q3=Quartile 3: 75% of women had ≤ this number of days of unscheduled bleeding |
|||||
|
91-Day Treatment Cycle |
Days per 84-Day Interval |
Days per 28-Day Interval |
|||
|
Q1 |
Median |
Q3 |
Mean |
Mean |
|
|
1st |
1 |
4 |
10 |
6.9 |
1.7 |
|
4th |
0 |
1 |
4 |
3.2 |
0.8 |
| Q1=Quartile 1: 25% of women had ≤ this number of days of unscheduled spotting Median: 50% of women had ≤ this number of days of unscheduled spotting Q3=Quartile 3: 75% of women had ≤ this number of days of unscheduled spotting. |
|||||||||||
|
91-Day Treatment Cycle |
Days per 84-Day Interval |
Days per 28-Day Interval |
|||||||||
|
Q1 |
Median |
Q3 |
Mean |
Mean |
|||||||
|
1st |
1 |
4 |
11 |
7.4 |
1.9 |
||||||
|
4th |
0 |
2 |
7 |
4.4 |
1.1 |
||||||
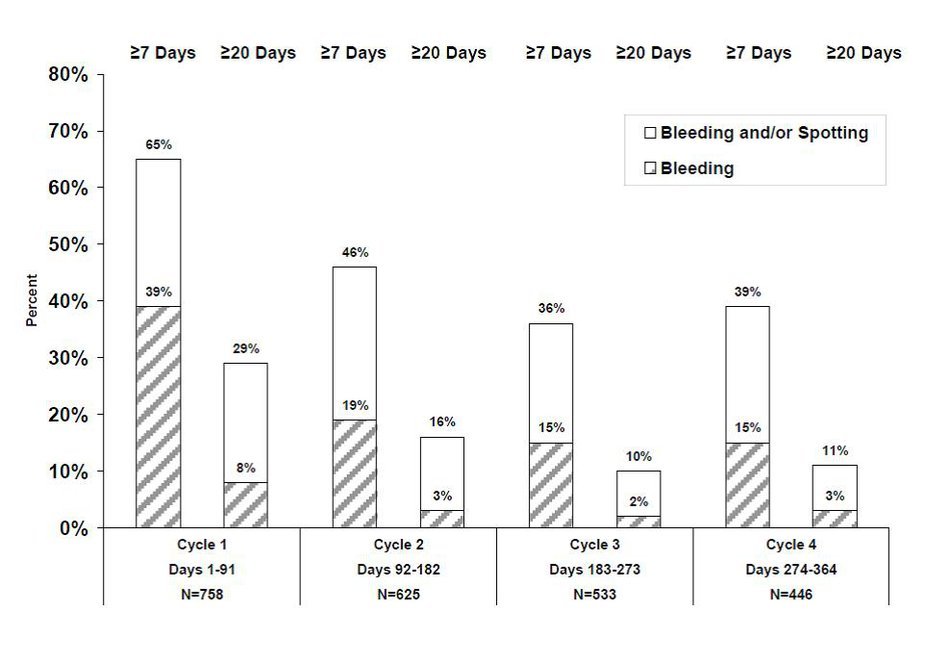
Figure 1 shows the percentage of levonorgestrel/ethinyl estradiol and ethinyl estradiol subjects participating in trial PSE-301 with ≥ 7 days or ≥ 20 days of unscheduled bleeding and/or spotting, or only unscheduled bleeding, during each 91-day treatment cycle.
Figure 1. Percent of Women Taking Levonorgestrel/Ethinyl Estradiol and Ethinyl Estradiol who Reported Unscheduled Bleeding and/or Spotting or only Unscheduled Bleeding
Amenorrhea sometimes occurs in women who are using COCs. Pregnancy should be ruled out in the event of amenorrhea. Some women may encounter amenorrhea or oligomenorrhea after stopping COCs, especially when such a condition was pre-existent.
COC Use Before or During Early Pregnancy
Extensive epidemiological studies have revealed no increased risk of birth defects in women who have used oral contraceptives prior to pregnancy. Studies also do not suggest a teratogenic effect, particularly in so far as cardiac anomalies and limb-reduction defects are concerned, when taken inadvertently during early pregnancy. Oral contraceptive use should be discontinued if pregnancy is confirmed.
The administration of oral contraceptives to induce withdrawal bleeding should not be used as a test for pregnancy
Emotional Disorders
Women with a history of depression should be carefully observed and Jaimiess discontinued if depression recurs to a serious degree.
Interference with Laboratory Tests
The use of COCs may change the results of some laboratory tests, such as coagulation factors, lipids, glucose tolerance, and binding proteins. Women on thyroid hormone replacement therapy may need increased doses of thyroid hormone because serum concentrations of thyroid binding globulin increase with use of COCs.
Monitoring
A woman who is taking COCs should have a yearly visit with her healthcare provider for a blood pressure check and for other indicated health care.
Other Conditions
In women with hereditary angioedema, exogenous estrogens may induce or exacerbate symptoms of angioedema. Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation while taking COCs.
Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to the rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The clinical trial that evaluated the safety and efficacy of levonorgestrel/ethinyl estradiol and ethinyl estradiol was a 12-month, randomized, multicenter, open-label study, which enrolled women aged 18-40, of whom 1,006 took at least one dose of levonorgestrel/ethinyl estradiol and ethinyl estradiol.
Adverse Reactions Leading to Study Discontinuation
16.3% of the women discontinued from the clinical trial due to an adverse reaction; the most common adverse reactions (≥ 1% of women) leading to discontinuation were irregular and/or heavy uterine bleeding (5.9%), weight gain (2.4%), mood changes (1.5%), and acne (1.0%).
Common Treatment-Emergent Adverse Reactions (≥ 5% of women)
Irregular and/or heavy uterine bleeding (17%), weight gain (5%), acne (5%).
Serious Adverse Reactions
Migraine, cholecystitis, cholelithiasis, pancreatitis, abdominal pain, and major depressive disorder.
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of levonorgestrel/ethinyl estradiol and ethinyl estradiol. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency of establish a causal relationship to drug exposure.
Gastrointestinal disorders: abdominal distension, vomiting
General disorders and administration site conditions: chest pain, fatigue, malaise, edema peripheral, pain
Immune system disorders: hypersensitivity reaction
Investigations:blood pressure increased
Musculoskeletal and connective tissue disorders: muscle spasms, pain in extremity
Nervous system disorders: dizziness, loss of consciousness
Psychiatric disorders: insomnia
Reproductive and breast disorders: dysmenorrhea
Respiratory, thoracic and mediastinal disorders: pulmonary embolism, pulmonary thrombosis
Skin and subcutaneous tissue disorders: alopecia
Vascular disorders: thrombosis
Drug Interactions
No drug-drug interaction studies were conducted with Jaimiess.
Changes in Contraceptive Effectiveness Associated with Co-Administration of Other Products
If a woman on hormonal contraceptives takes a drug or herbal product that induces enzymes, including CYP3A4, that metabolize contraceptive hormones, counsel her to use additional contraception or a different method of contraception. Drugs or herbal products that induce such enzymes may decrease the plasma concentrations of contraceptive hormones, and may decrease the effectiveness of hormonal contraceptives or increase breakthrough bleeding. Some drugs or herbal products that may decrease the effectiveness of hormonal contraceptives include:
barbiturates
bosentan
carbamazepine
felbamate
griseofulvin
oxcarbazepine
phenytoin
rifampin
St. John’s wort
topiramate
HIV protease inhibitors and non-nucleoside reverse transcriptase inhibitors: Significant changes (increase or decrease) in the plasma levels of the estrogen and progestin have been noted in some cases of co-administration of HIV protease inhibitors or with non-nucleoside reverse transcriptase inhibitors.
Antibiotics: There have been reports of pregnancy while taking hormonal contraceptives and antibiotics, but clinical pharmacokinetic studies have not shown consistent effects of antibiotics on plasma concentrations of synthetic steroids.
Consult the labeling of all concurrently-used drugs to obtain further information about interactions with hormonal contraceptives or the potential for enzyme alterations.
Increase in Plasma Levels of Estradiol Associated with Co-Administered Drugs
Co-administration of atorvastatin and certain COCs containing ethinyl estradiol increase AUC values for ethinyl estradiol by approximately 20%. Ascorbic acid and acetaminophen may increase plasma ethinyl estradiol levels, possibly by inhibition of conjugation. CYP3A4 inhibitors such as itraconazole or ketoconazole may increase plasma hormone levels.
Concomitant Use with Hepatitis C Vaccine (HCV) Combination Therapy – Liver Enzyme Elevation
Do not co-administer Jaimiess with HCV drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to potential for ALT elevations
Changes in Plasma Levels of Co-Administered Drugs
COCs containing some synthetic estrogens (e.g., ethinyl estradiol) may inhibit the metabolism of other compounds. COCs have been shown to significantly decrease plasma concentrations of lamotrigine likely due to induction of lamotrigine glucuronidation. This may reduce seizure control; therefore, dosage adjustments of lamotrigine may be necessary. Consult the labeling of the concurrently-used drug to obtain further information about interactions with COCs or the potential for enzyme alterations.
USE IN SPECIFIC POPULATIONS
Pregnancy
There is little or no increased risk of birth defects in women who inadvertently use COCs during early pregnancy. Epidemiologic studies and meta-analyses have not found an increased risk of genital or non-genital birth defects (including cardiac anomalies and limb-reduction defects) following exposure to low dose COCs prior to conception or during early pregnancy.
The administration of COCs to induce withdrawal bleeding should not be used as a test for pregnancy. COCs should not be used during pregnancy to treat threatened or habitual abortion.
Women who do not breastfeed may start COCs no earlier than four to six weeks postpartum.
Nursing Mothers
When possible, advise the nursing mother to use other forms of contraception until she has weaned her child. Estrogen-containing COCs can reduce milk production in breastfeeding mothers. This is less likely to occur once breastfeeding is well established; however, it can occur at any time in some women. Small amounts of oral contraceptive steroids and/or metabolites are present in breast milk.
Pediatric Use
Safety and efficacy of Jaimiess have been established in women of reproductive age. Safety and efficacy are expected to be the same for postpubertal adolescents under the age of 18 as for users 18 years and older. Use of Jaimiess before menarche is not indicated.
Geriatric Use
Jaimiess has not been studied in women who have reached menopause and is not indicated in this population.
Hepatic Impairment
No studies have been conducted to evaluate the effect of hepatic disease on the disposition ofJaimiess. However, steroid hormones may be poorly metabolized in patients with impaired liver function. Acute or chronic disturbances of liver function may necessitate the discontinuation of COC use until markers of liver function return to normal. [See 142 and 35.34].
Renal Impairment
No studies have been conducted to evaluate the effect of renal disease on the disposition of Jaimiess.
Overdosage
There have been no reports of serious ill effects from overdose of oral contraceptives, including ingestion by children. Overdosage may cause withdrawal bleeding in females and nausea.
Jaimiess Description
Jaimiess is an extended-cycle oral contraceptive consisting of 84 peach tablets each containing 0.15 mg of levonorgestrel, a synthetic progestogen and 0.03 mg of ethinyl estradiol, and 7 yellow tablets containing 0.01 mg of ethinyl estradiol.
The structural formulas for the active components are:
Levonorgestrel is chemically 18,19-Dinorpregn-4-en-20-yn-3-one, 13-ethyl-17-hydroxy-, (17α)-, (-)-.
Ethinyl Estradiol is 19-Norpregna-1,3,5(10)-trien-20-yne-3,17-diol, (17α)-.
Each peach tablet contains the following inactive ingredients: anhydrous lactose, iron oxide black, iron oxide red, iron oxide yellow, magnesium stearate, povidone, polyethylene glycol, polyvinyl alcohol-part hydrolyzed, talc, and titanium dioxide.
Each yellow tablet contains the following inactive ingredients: iron oxide yellow, lactose monohydrate, lecithin, magnesium stearate, microcrystalline cellulose, polyvinyl alcohol, talc, titanium dioxide and xanthan gum.
Jaimiess - Clinical Pharmacology
Mechanism of action
COCs lower the risk of becoming pregnant primarily by suppressing ovulation. Other possible mechanisms may include cervical mucus changes that inhibit sperm penetration and endometrial changes that reduce the likelihood of implantation.
Pharmacokinetics
Absorption
Ethinyl estradiol and levonorgestrel are absorbed with maximum plasma concentrations occurring within 2 hours after ethinyl estradiol and levonorgestrel administration. Levonorgestrel is completely absorbed after oral administration (bioavailability nearly 100%) and is not subject to first-pass metabolism. Ethinyl estradiol is absorbed from the gastrointestinal tract but, due to first-pass metabolism in gut mucosa and liver, the bioavailability of ethinyl estradiol is approximately 43%.
The daily exposure to levonorgestrel and ethinyl estradiol on Day 21, corresponding to the end of a typical 3-week contraceptive regimen, and on Day 84, at the end of an extended cycle regimen, were similar. There was no additional accumulation of ethinyl estradiol after dosing a 0.03 mg ethinyl estradiol tablet during Days 84-91. The mean plasma pharmacokinetic parameters of ethinyl estradiol and levonorgestrel following a single dose of one levonorgestrel/ethinyl estradiol combination tablet, for 84 days, in normal healthy women are reported in Table 3.
|
|
AUC0-24 hr |
Cmax |
Tmax |
|
Levonorgestrel |
|||
|
Day 1 |
18.2 ± 6.1 ng•hr/mL |
3.0 ± 1.0 ng/mL |
1.3 ± 0.4 hours |
|
Day 21 |
64.4 ± 25.1 ng•hr/mL |
6.2 ± 1.6 ng/mL |
1.3 ± 0.4 hours |
|
Day 84 |
60.2 ± 24.6 ng•hr/mL |
5.5 ± 1.6 ng/mL |
1.3 ± 0.3 hours |
|
Ethinyl Estradiol |
|||
|
Day 1 |
509.3 ± 172.0 pg•hr/mL |
69.8 ± 26 pg/mL |
1.5 ± 0.3 hours |
|
Day 21 |
837.1 ± 271.2 pg•hr/mL |
99.6 ± 31 pg/mL |
1.5 ± 0.3 hours |
|
Day 84 |
791.5 ± 215.0 pg•hr/mL |
91.3 ± 32 pg/mL |
1.6 ± 0.3 hours |
The effect of food on the rate and the extent of levonorgestrel and ethinyl estradiol absorption following oral administration of Jaimiess has not been evaluated.
Distribution
The apparent volume of distribution of levonorgestrel and ethinyl estradiol are reported to be approximately 1.8 L/kg and 4.3 L/kg, respectively. Levonorgestrel is about 97.5 to 99% protein-bound, principally to sex hormone binding globulin (SHBG) and, to a lesser extent, serum albumin. Ethinyl estradiol is about 95 to 97% bound to serum albumin. Ethinyl estradiol does not bind to SHBG, but induces SHBG synthesis, which leads to decreased levonorgestrel clearance. Following repeated daily dosing of levonorgestrel/ethinyl estradiol oral contraceptives, levonorgestrel plasma concentrations accumulate more than predicted based on single-dose pharmacokinetics, due in part, to increased SHBG levels that are induced by ethinyl estradiol, and a possible reduction in hepatic metabolic capacity.
Metabolism
Following absorption, levonorgestrel is conjugated at the 17β-OH position to form sulfate and to a lesser extent, glucuronide conjugates in plasma. Significant amounts of conjugated and unconjugated 3α,5β-tetrahydrolevonorgestrel are also present in plasma, along with much smaller amounts of 3α,5α-tetrahydrolevonorgestrel and 16β-hydroxylevonorgestrel. Levonorgestrel and its phase I metabolites are excreted primarily as glucuronide conjugates. Metabolic clearance rates may differ among individuals by several-fold, and this may account in part for the wide variation observed in levonorgestrel concentrations among users.
First-pass metabolism of ethinyl estradiol involves formation of ethinyl estradiol-3-sulfate in the gut wall, followed by 2-hydroxylation of a portion of the remaining untransformed ethinyl estradiol by hepatic cytochrome P-450 3A4 (CYP3A4). Levels of CYP3A4 vary widely among individuals and can explain the variation in rates of ethinyl estradiol hydroxylation. Hydroxylation at the 4-, 6-, and 16- positions may also occur, although to a much lesser extent than 2-hydroxylation. The various hydroxylated metabolites are subject to further methylation and/or conjugation.
Excretion
About 45% of levonorgestrel and its metabolites are excreted in the urine and about 32% are excreted in feces, mostly as glucuronide conjugates. The terminal elimination half-life for levonorgestrel after a single dose of ethinyl estradiol and levonorgestrel was about 34 hours.
Ethinyl estradiol is excreted in the urine and feces as glucuronide and sulfate conjugates, and it undergoes enterohepatic recirculation. The terminal elimination half-life of ethinyl estradiol after a single dose of levonorgestrel/ethinyl estradiol and ethinyl estradiol was found to be about 18 hours.
Race
The effect of race on the pharmacokinetics of Jaimiess has not been evaluated.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment of Fertility
Clinical Studies
In a 12-month, multicenter, randomized, open-label clinical trial, 1,006 women aged 18-40 were studied to assess the safety and efficacy of ethinyl estradiol and levonorgestrel, completing the equivalent of 8,681 28-day cycles of exposure. The racial demographic of those enrolled was: Caucasian (80%), African-American (11%), Hispanic (5%), Asian (2%), and Other (2%). There were no exclusions for body mass index (BMI) or weight. The weight range of those women treated was 91 to 360 lbs., with a mean weight of 156 lbs. Among the women in the trial, 63% were current or recent hormonal contraceptive users, 26% were prior users (who had used hormonal contraceptives in the past but not in the 6 months prior to enrollment), and 11% were new starts. Of treated women, 14.8% were lost to follow-up, 16.3% discontinued due to an adverse event, and 12.9% discontinued by withdrawing their consent.
The pregnancy rate (Pearl Index [PI]) in women aged 18-35 years was 1.34 pregnancies per 100 women-years of use (95% confidence interval 0.54-2.75), based on 7 pregnancies that occurred after the onset of treatment and within 14 days after the last combination pill. Cycles in which conception did not occur, but which included the use of backup contraception, were not included in the calculation of the PI. The PI includes patients who did not take the drug correctly.
How Supplied/Storage and Handling
How Supplied
Jaimiess (levonorgestrel/ethinyl estradiol tablets, USP and ethinyl estradiol tablets, USP) are available in Extended-Cycle Tablet Dispensers, each containing a 13-week supply of tablets: 84 peach tablets, each containing 0.15 mg of levonorgestrel and 0.03 mg ethinyl estradiol, and 7 yellow tablets each containing 0.01 mg of ethinyl estradiol. The peach tablets are round, film-coated, debossed with SZ on one side and J4 on the other side. The yellow tablets are round, film-coated, debossed with SZ on one side and L1 on the other side.
NDC 70700-123-87 (1 extended-cycle tablet dispenser, each tablet dispenser contains 91 tablets)
Storage Conditions
Store at 20° to 25° C (68° to 77° F) [See USP Controlled Room Temperature].
Patient Counseling Information
Counsel patients that cigarette smoking increases the risk of serious cardiovascular events from COC use, and that women who are over 35 years old and smoke should not use COCs.
Counsel patients that this product does not protect against HIV-infection (AIDS) and other sexually transmitted diseases.
Counsel patients on Warnings and Precautions associated with COCs.
Counsel patients to take one tablet daily by mouth at the same time every day. Instruct patients what to do in the event pills are missed. See WHAT TO DO IF YOU MISS PILLS section of FDA-Approved Patient Labeling.
Counsel patients to use a back-up or alternative method of contraception when enzyme inducers are used with COCs.
Counsel patients who are breastfeeding or who desire to breastfeed that COCs may reduce breast milk production. This is less likely to occur if breastfeeding is well established.
Counsel any patient who starts COCs postpartum, and who has not yet had a period, to use an additional method of contraception until she has taken a light blue-green tablet for 7 consecutive days.
Counsel patients that amenorrhea may occur. Pregnancy should be considered in the event of amenorrhea, and should be ruled out if amenorrhea is associated with symptoms of pregnancy, such as morning sickness or unusual breast tenderness.